Today was my last day of medical school classes. Four years, lots of friends, lots of memories, and a lot of fun. It was tiring, it was invigorating, it was exhausting, and overall it was pretty incredible. As approach actually getting my doctorate, the one thing I’ll take away is that I will always be a learner. I hope I’ll always learn new things, and be open to learning new things. That’s what makes medicine so appealing to me. So to commemorate the end of my “classes” aspect of medicine, I wanted to start a Mini-Medicine series. A few posts where I mostly review topics for myself, but hopefully they can be informative for others as well. Hopefully there will be more to come!
—-
Hiking is fun. I would say I’m an a novice hiker. Before we went to Peru, I was solidly in the novice category: I like doing it, but honestly it’s a little scary to watch my technique going down hill. After arguably the scariest thing I’ve ever done by hiking on a gravelly, highly inclined surface just inches away from a plunge into the rushing river below in Cotahuasi Canyon, I feel like I can say I’ve moved up a level into novice-to-moderate. Woo!
As we were going along though, I kept thinking about hiking at altitude: what happens to your body, why you get so exhausted, and why it makes you sick. Honestly, it’s tough…hiking at altitude is just a totally different beast, an exhausting beast. So after hearing my friend Jill talk about her hike on Mt. Kilimanjaro at 20k feet, I figured I should do a quick review for myself about what makes altitude physiology so cool, different, and exhausting.
What is considered high altitude? What is altitude sickness?
There’s a handy dandy scale that we can use to describe how “high” we are going:
 Altitude sickness is what happens when you can’t get enough oxygen to your body, and it starts to let you know through headaches, disturbed sleep, loss of appetite, confusion, etc. For those that ignore the warning signs, it can sometimes be really dangerous.
Altitude sickness is what happens when you can’t get enough oxygen to your body, and it starts to let you know through headaches, disturbed sleep, loss of appetite, confusion, etc. For those that ignore the warning signs, it can sometimes be really dangerous.
Two common misconceptions I came across when doing my research: it has nothing to do with your starting fitness level, or being a woman. There is no data to support these claims as of yet.
What happens to air as you go higher and higher above sea level?
It’s important to understand what makes up air in general. All air, no matter where you are is ~21% oxygen (O2) and the rest is mostly nitrogen and a few other gasses. No matter where you are in our atmosphere, the percent of oxygen in the air will always be 21%.
So when you go higher and higher, the percent make up of gases around you doesn’t change, but the pressure of the gases around you goes down. So by the time you are at 15,000 ft, the pressure of all the air around you is WAY less than it was before, around 43% less pressure than you feel at sea level.
That’s what people mean when they say the air is “thinner” at altitude — you have less air pressure on you. It’s not that there is less oxygen relative to the other gases, that stays the same at 21% of the total gases, but it’s that there are fewer air molecules when you’re high up in general.
Partial Pressures
With air, the gases that exert pressure on us (air pressure/atmospheric pressure) are mostly nitrogen and oxygen. The “partial pressure” is the pressure of each gas alone. So the partial pressure of oxygen, is the pressure that just oxygen creates by itself. Since our body cares about oxygen a LOT, the pressure of O2 is super important.

The partial pressure of each gas individually is the partial pressure, and it sum of the partial pressure makes up the total pressure. This image was taken from Khan Academy, which adapted it from OpenStax, CCBY 3.0
Why does lower air pressure matter when it comes to oxygen getting into your body?
The way oxygen gets into our bloodstream from our lungs all comes down to pressure. If the pressure of oxygen in the air is higher than the pressure of oxygen dissolved in your bloodstream, then it will move down its concentration gradient, going from high O2 to low O2.
When you are at sea level, the partial pressure of oxygen is much higher than the pressure of oxygen in your body. So when you breathe in, the oxygen in your lungs is at a higher pressure than the oxygen in your bloodstream and we fully oxygenated our blood. This pressure difference is the only driving force getting oxygen into your blood.
The higher the pressure difference (like if I were to put a pure oxygen mask on your face), the higher the gradient, the more oxygen dissolves into your plasma.
At altitude, you have less pressure in general, so the partial pressure of O2 is lower, sometimes waaaaaay lower than at sea level. So that gradient pushing oxygen into your blood isn’t as big, so you’re not “pushing” oxygen molecules into your blood as hard. This is why when you get to altitude you get that short of breath feeling after just taking a few steps: you actually have less oxygen in your body.
How is the partial pressure of oxygen related to hemoglobin saturation with oxygen?
Now we get to the graph that set me down my path towards becoming an anesthesiologist: the oxygen-hemoglobin dissociation curve. This just means that there is a relationship between the pressure of oxygen in your bloodstream and the amount of oxygen attached to hemoglobin.
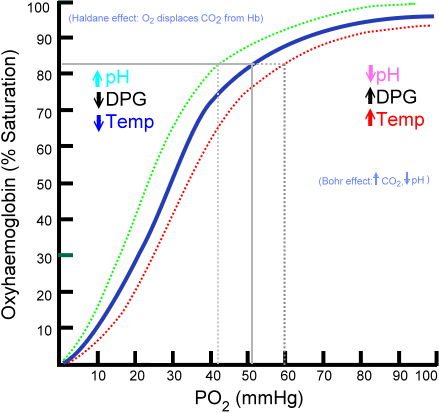
Saturation of hemoglobin is dependent on the partial pressure of oxygen in the arterial blood. The shape is non-linear due to properties of the hemoglobin molecule. The plain blue line is the “normal” curve. Image taken from wikipedia.
What this curve it’s showing is that after a certain partial pressure of oxygen, around 90 mmHg or so, there is not much gain in the saturation of hemoglobin molecules (the curve flattens out). But below a certain pressure, around 50-60 mmHg, around where the curve becomes closer to linear, for every small change in pressure, there is a dramatic change in hemoglobin saturation…meaning there’s a lot less oxygen attached to the hemoglobin, and a lot less oxygen going to your vital organs…like your brain.
Example time, aka putting it all together
 Consider my friend Jill again on Mt. Kilimanjaro. Starting at sea level, she is experiencing 760 mmHg of air pressure, which is what she breathes in. As it’s coming in, the air is warmed and humidified, so water vapor replaces some of the air molecules, so the pressure of air coming in is now 713 mmHg. Of that, 21% is still oxygen, which brings the oxygen she’s breathing in to around 150 mmHg, and then because of more displacement along the way, the oxygen that hits her lung is around 105 mmHg.
Consider my friend Jill again on Mt. Kilimanjaro. Starting at sea level, she is experiencing 760 mmHg of air pressure, which is what she breathes in. As it’s coming in, the air is warmed and humidified, so water vapor replaces some of the air molecules, so the pressure of air coming in is now 713 mmHg. Of that, 21% is still oxygen, which brings the oxygen she’s breathing in to around 150 mmHg, and then because of more displacement along the way, the oxygen that hits her lung is around 105 mmHg.

Jill on Kilimanjaro at 20,000 ft!
So the deoxygenated blood that comes back to her heart after feeding her body is at around 40 mmHg of oxygen…so that’s a pretty big gradient, 105 mmHg in her lungs –> 40 mmHg in her blood…so oxygen diffuses down this gradient until it equalizes, so the blood leaving her heart and getting pumped out to her body is…viola at 100 mmHg, replenished and ready to fuel oxidative phosphorylation! Woo!
Now imagine she’s on Kilimanjaro at 20,000 feet where she experiences about 349 mmHg of air pressure…less than half of what she gets at sea level! Doing some math, that makes the oxygen in the air around 63 mmHg, making it even less in your lungs, likely around 44-55 mmHg, depending on how fast she is breathing — the faster she breaths, the higher the partial pressure of oxygen will be…which is why you breathe fast**! Anyways, looking up at the oxygen-hemoglobin dissociation curve, you can see that at 50 mmHg, her hemoglobin saturation is around 80-85%. In an acute change situation (i.e. going from 100% saturation –> 80% in a matter of a few days) this can be pretty bad. Your body, especially your brain which is very oxygen sensitive, is not set up to handle this. This is why you get sleepy, tired, and confused at high altitudes. This is one of the main symptoms of altitude sickness.
**When you have really low oxygen, you get a trigger from your brain to breathe faster. This is an attempt to increase the partial pressure of oxygen in your lungs (and therefore in your bloodstream). This works by essentially breathing more so that you replace used up residual air in your lungs with “new,” and therefore higher oxygen, air.
Dangerous Parts of Altitude Sickness
Two of the big things to be concerned about are HACE and HAPE. HACE = high altitude cerebral edema, and HAPE = high altitude pulmonary edema. Let me start by saying there is no definitive answer as to how these things happen, but we just know that they are more common if you ascend quickly without allowing your body to acclimate to low oxygen.

Chest X-ray showing pulmonary edema aka excess fluid in the lungs. The circle and arrow show you the examples of the fluid. Image taken from wikipedia.
HAPE: The current hypothesis is that the low oxygen leads to your blood vessels in your lungs to constrict and squeeze out excess fluid. Obviously then…your lungs can’t exchange gas, and that’s a major problem. The symptoms typically include severe shortness of breath persistent at rest, cough, maybe pink/frothy stuff (sputum) coming up from your lungs.
HACE: We seem to know even less about what causes this, with the predominant thought that low oxygen leads to the blood vessels in your brain to dilate and makes them pathologically leaky…which allows fluid to go into your brain, making it swell. The main symptoms of this are severe headache, nausea, unsteady walking/gait, and change in mental status (i.e. way sleepier, problems with train of thought, etc).
These serious complications of altitude sickness can usually be staved off by allowing your body to acclimate as you go higher, basically a slow and steady pace…and also listening to your body. If you are not feeling well do not continue to go up. Wait a day or so, allow your body to acclimate to the lower oxygen, and then continue to go up. With altitude sickness, there is no such thing as “powering through.”
That’s it for the first Mini-Medicine post…hopefully there will be more! As always, this is not to be taken as individual medical advice. If you have medical questions, please seek out your own health care provider. If you have any questions/comments/additions/corrections, please comment below. Special thanks to Amy Holmstrom and Tyler who chatted physiology out with me. Thanks to Jill for letting me turn her into a stick figure in my post.

{kind=link}
Chewing the leaves of the coca plant or taking the homeopathic Coca has been shown to improve your body’s ability to adapt.
LikeLike
Hey Valeria! Thank you for commenting — Tyler and I used Coca leaves while in Peru to help dampen the symptoms of altitude sickness, and we felt that they helped us stay awake! I could not find any papers showing that they actually helped the body adapt — please share those with me if you have a moment, I would love to read them 🙂
LikeLike
Keep up the good work. It made enjoyable and informative reading.
LikeLike